
The Sweetest Poisons: Part 10B
Sex ratios, detransition, and increasing numbers of trans teenagers
Let’s get started again with the same quote from Julia Serano1:
…if trans people are imagined to be “contaminating” and capable of “infecting” or “converting” others (whether via “social contagion” or “grooming”), then that provides a convenient excuse for those who wish to “quarantine” us (e.g., by preventing us from participating in society, censoring our life experiences and perspectives, or perhaps even eliminating us all together).
Julia Serano - “All the Evidence Against Transgender Social Contagion”
Note on this post: This is part of a series, started by my friend Billie Hoard discussing Dr. Preston Sprinkle’s book Embodied. You can see the whole index for the series here. If you haven’t already, you’ll want to read at least the previous entry, covering the first part of this chapter. To recap, I discussed how the entire concept of Rapid-Onset Gender Dysphoria (ROGD) is junk science (technical term), not to be taken seriously. I also discussed Dr. Sprinkle’s first example — a woman who detransitioned — and how he forces her story to fit his narrative more neatly.
We begin immediately after where we left off. Dr. Sprinkle concludes Helena’s story of transition and detransition. After issuing the reminder that, “We should never view an entire idea or concept through the lens of just one story,” he says the following,
But in the last few years, stories like Helena’s have exploded on the scene.2
No citation is given. No source. It’s not quantified, and therefore is difficult to refute directly.
I will grant that the rising number of people transitioning almost certainly increases the number of people detransitioning, because increasing the number of people who do a thing pretty much always increases the number of people who regret doing that thing.
But we do not gauge risk based on absolute quantity (which, again, Dr. Sprinkle doesn’t even provide here), but rather on likelihood. It’s not enough to know that a treatment can go wrong, you want to know the odds. Then, a patient weighs risks and benefits, gathering the needed information.
This is why it’s so critical to understand that, as I said last time, 94% of transitioners are more satisfied with their life now, while less than 3% are less satisfied.3 True regret was found to be roughly 1% in a 2023 review including, “27 studies involving almost 8,000 teens and adults who had transgender surgeries”4.
Dr. Sprinkle’s use of the word “exploded” here is a poor choice, since it creates a clear impression for the reader, which is neither contextualized nor backed by data he shares. Someone who is interested in facts should strive for dispassionate language5.
Moving forward, he says this:
Some call the sudden rise of dysphoria in teens a trend. Others call it an outbreak.[4]6. Some psychologists have termed it Rapid-Onset Gender Dysphoria (ROGD).
First, there is no evidence that there is a rise of dysphoria in teens. There is a rise in rates of diagnosis of gender dysphoria, but one need only look at my own story to know that many cases of gender dysphoria were undiagnosed in the past. We’ll talk more about this later in this essay.
Only one source is given for his claim here, which is to an article written in October 2017 by Lisa Marchiano.7 The earliest known use of the phrase was by Dr. Lisa Littman (MD, Residency in Ob/Gyn), including on a site now known to be run by Marchiano.8 Dr. Littman’s heavily corrected 2018 paper includes “Rapid-Onset Gender Dysphoria” in the title. The paper has no co-authors, but gives three acknowledgements for assistance with the paper, one of which is for Lisa Marchiano.
Neither Marchiano nor Dr. Littman had professionally worked with transgender children9, and neither claims to be a psychologist.
Again, Dr. Sprinkle’s characterization, at least given the sources he has cited, inflates the number of individuals and appears to invent their credentials.
Dr. Sprinkle’s use of the loaded terms “sudden” and “outbreak” also cultivate a sense of “something is wrong” in the reader before he’s ever even introduced the facts.
However, prior to Dr. Sprinkle jumping into the study, he drops in a few common talking points that we need to address.
The Increase
Sprinkle goes on to say:
Whatever you name it, the percentage of teenagers identifying as trans*—a growing number of whom later detransition—has risen exponentially, especially among female teenagers.
Again, no citation for the growth in trans teens is given, but it is accurate that more teens are identifying as transgender or non-binary. A Reuters report from 2022 showed that new diagnoses of gender dysphoria among youth aged 6-17 increased from roughly 15,000 in 2017 to roughly 42,000 in 2021.10 For context, as the report states, there are roughly 48 million people in the US in that age range. If we take the total of 121,882 in that five year period, we find that roughly 0.3% of them received a diagnosis. Of those, just 17,683 (15%) received puberty blockers, hormones, or both, representing just 0.037% (one in roughly 2,700) of the total youth population studied11.
On the other hand, a 2024 study12 found that “About 3.3% of high school students identify as transgender and another 2.2% have at some point questioned if they were.” Using the lower number (3.3%), and comparing it to the percent receiving puberty blockers and hormones, we can say that just 1.1% (one in 89) of those who identify as transgender are currently seeking medical care13. That’s important, because most concerns around transition center around fears of medical interventions doing “irreversible damage”14. But this data shows that nearly all trans high schoolers are only socially transitioning, in which they might change their name, pronouns, or choices like clothing and hairstyle. For these youth, were they to ultimately identify with their assigned sex at birth, there’s no permanent changes made.
Detransition
I will grant that “a growing number of whom later detransition” (emphasis mine) is likely accurate. But the raw number of people who detransition is hardly interesting. That’s like saying that, since the introduction of the iPhone in 2007, “a growing number of people are returning their iPhones”. Almost certainly true, but simply because the number of people buying iPhones increases. As more people buy them, the inevitable return count increases, even if (if Apple is doing quality control well), the percentage may have decreased.
The relevant statistic is whether or not the percentage of individuals detransitioning is increasing, and (again), Dr. Sprinkle doesn’t give a citation. However, even the UK’s Cass Review (not peer-reviewed), published in 2024, seen by many as having significant anti-trans bias15, found that “less than ten” of the 3,499 cases they tracked of youth being treated for gender dysphoria resulted in detransition. That’s a maximum rate of just 0.3%. Anti-trans voices have been speculating about rising detransition rates for quite some time now16, but they simply have not materialized1718.
These rates, as many point out, are far better than many common medical interventions. A 2024 study in the American Journal of Surgery19 found that regret for gender-affirming surgery was less than 1%, while it was significantly higher for other types of surgery, including breast reconstruction, breast augmentation, prostatectomy, and bariatric surgery. It also found that regret rate for some life decisions was significantly higher, including 7% who regret having children. 43% of first marriages end in divorce, and divorce is the end of a whopping 73% of third marriages20.
In conclusion, not only do a low percentage of those who transition eventually detransition, but that percentage is significantly lower than for other common medical interventions and life decisions.
Sex Ratio Among Transgender Youth
Dr. Sprinkle claims (again, with no source) that this increase is found “especially among female teenagers.” First, he should have said “transgender teen boys”, rather than misgendering them as “female.” Second, a 2022 study published in Pediatrics (“The Official Journal of the American Academy of Pediatrics”) by Dr. Jack Turban21 and others found that, as of 2019, the sex ratio amongst transgender youth in the US was roughly 1.2 trans feminine teens for every trans masculine teen. That is a decrease in ratio from 1.5 found in 2017. There has been a larger increase amongst trans masculine teens seeking medical care (remember, this is a small subset of those who identify as transgender) in the UK, now exceeding the number of trans feminine teens.
Julia Serano, as always, has an excellent article22 diving into the discussion, but I want to highlight a few things here.
First, why is this bad? If there was no concern about there being more trans femme individuals before, then why is there concern about there being more trans masc individuals now (if indeed there are)? Why must there be more trans femmes than trans mascs?
If you pay attention to trans discourse as much as I do, you’ll see that the conversation is dominated by concerns about trans women (adults) and trans boys (youth). Adult trans men are frequently completely forgotten about, and trans girls (youth) are also frequently ignored. Trans women are cast as deviant men, or even a threat. Trans boys, on the other hand, are cast as impressionable young girls; hapless victims of “gender ideology.”
As Serano writes, it’s hard not to believe that this is partially rooted in cultural misogyny that infantilizes teen “girls”, and shames feminine “men”. In more patriarchal circles where women’s primary role is to bear children, this can take on the appearance of a panic about the potential for trans boys to lose their fertility. First, this is not an inevitable result of transition, especially if no medical interventions occur. Remember, gender confirmation surgery (genital surgery or removal of reproductive organs) for minors is an incredibly rare thing in the United States - performed less than 20 times per year23.
But additionally, there is simply no reason to believe that the sex ratios from 15 years ago were the “true ratio”, when so few trans people were able to be “out.” It’s better, in my opinion, to see early data on sex ratios as a small and skewed sample size, and that we will learn more as we go forward.
Setup for ROGD Discussion
Dr. Sprinkle then writes something of his goal for the coming pages:
I want to discuss this social phenomenon, since it raises many practical questions about trans* identities, mental health, online influence, and the ethics of medical interventions for adolescents. Let’s first get our minds around the recent escalation of teens identifying as trans*.
As we covered, there is no “social phenomenon” of ROGD, and therefore it cannot raise any questions. But let’s see what Dr. Sprinkle has to say.
“What is Rapid-Onset Gender Dysphoria?”
This is the next section header, and, as discussed, it’s nothing. I guess it could be said it’s a junk science term used to cast doubt on transgender identities and gender transition as a whole, but nothing more than that.
But first, he goes back to covering the increase in the percentage of youth identifying as transgender.
Fast Increase
Here’s how Dr. Sprinkle begins:
In many Western countries, we’ve seen a massive spike in teenagers questioning their gender. For instance, the Tavistock Centre in London, the main gender clinic in the United Kingdom, treated 51 (34 males, 17 females) children and teenagers in 2009 who had gender dysphoria or were identifying as trans*. In 2016, the same clinic saw 1,766 (557 males, 1,209 females) children and teenagers, and in 2019 it saw 2,364 (624 males, 1,740 females).[5]24 That’s more than a 5,000 percent increase among females in ten years.
These numbers are referring more specifically to the Gender Identity Development Service, which was based at the Tavistock Centre. In my time in trans discourse, these Tavistock numbers are brought up more than any others regarding “rapid increase”. Let’s take a look at them a little more closely.
First, according to the wikipedia article25 “Puberty blockers were considered a usable option by the end of the 1990s but only for patients aged 16 or over who had first tried extensive therapy.” This protocol appears to have held until 2011, when the following changes began:
In 2011, in response to changing international standards for gender care, the clinic began a research study allowing a "carefully selected group of young people" to receive puberty blockers after the age of 12. In 2014, prior to the study's completion, the clinic received NHS approval to offer them without mandating enrollment in a research study.[16] In 2012, the service was extended to a satellite site in Leeds. Endocrine support was also extended to Leeds Children's Hospital at the Leeds General Infirmary site in 2013.[17]
Also of note, the WPATH Standards of Care (which informs gender-affirming care across the world) version 7 were published in 2012.26
So 2009 is not a neutral starting point, from which we could expect only organic growth. Those numbers were under a very tightly controlled set of parameters. Instead, the potential age range tripled in 2011 (from 16-17 to 12-17), with barriers further reduced in each of 2012, 2013, and 2014.
So let’s look at those 2016-2019 numbers that Dr. Sprinkle cites. Among those assigned male at birth, the service saw an increase from 557 to 624 patients, or approximately 4% annualized growth. That’s hardly remarkable. For those assigned female at birth, the increase is from 1,209 to 1,740. That’s a 13% annual growth rate. More rapid, but hardly “exponential”, to borrow Dr. Sprinkle’s word from earlier in the chapter. The percentage of those assigned male at birth (which Dr. Sprinkle will discuss later) declined modestly from 31% to 26%.
Incidentally, in 2011, a survey was done on patient satisfaction, and it found this, again according to Wikipedia27:
In 2011, a patient satisfaction survey found the majority were satisfied, but a quarter expressed dissatisfaction with long wait lists. Other concerns included geographic inaccessibility and the requirement for real-life experience.[18]
Note that by then, there were already concerns about long wait lists, geographic inaccessibility, and the requirement for “real-life experience” (in which patients are required to socially transition prior to medical treatment), all of which would have suppressed the number of patients treated.
Despite all of that, according to the study analyzing those survey responses, “Ninety-four percent [of patients] would recommend the services if a friend or relative had a gender-related problem.”28
By 2021, wait lists had increased to over two years, longer in some other cases. I highly recommend watching this episode of Philosophy Tube (Abigail Thorn) about her experience, as an adult, trying to get gender-affirming care in the UK. It will dispel any notions that somehow the UK’s medical system was rushing people into gender-affirming care — quite the opposite was the case.
So yes, the numbers have increased, as happens when a new service is available, and then again when it’s made more accessible. But the increases in the most recent years for which data was presented show modest year-over-year growth, and the numbers are quite small when compared to population, having never reached more than one in a thousand children in that age range29.
Since the service was quite small prior to 2011, and COVID affected numbers in the 2020-21 and 2021-22 financial years, I’ve charted the referrals from 2011-12 to 2019-2020.

And here is the growth rate by year:
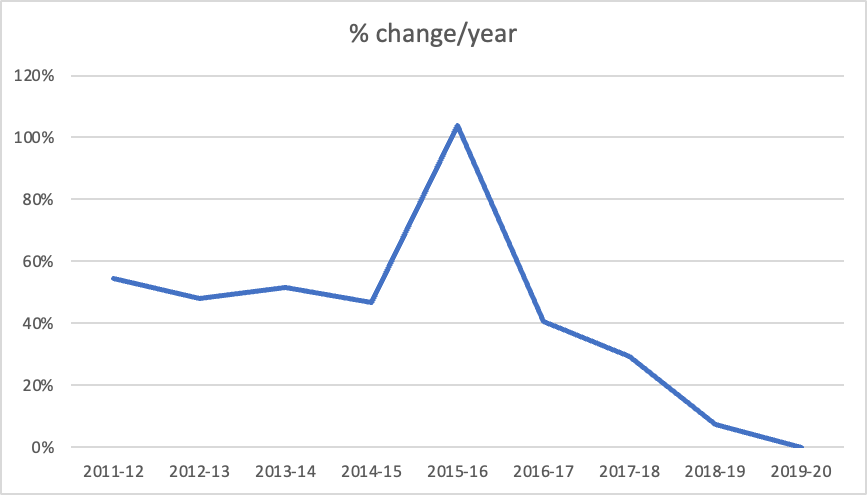
There was a single anomolous (from 2014-15 to 2015-16) year. Recall that, sometime in 2014, they stopped requiring patients to enroll in studies, making it much easier to access care. Other than that, growth rates in referrals per year had been falling quite steadily, actually reaching 7% in 2018-2019, and then 0% in 2019-2020’s Financial Year30.
And this is where I have to bring the left-handedness graph in. In the early 1900’s, left-handedness was stigmatized, and frequently children were forced to write with their right hand anyways. This caused significant psychological damage, and eventually children were allowed to use either hand.

Numbers start at 3%, and then “increase dramatically” to ~12% from roughly 1915 to 1940, a twenty-five year period. And then, of course, they level out. We can assume from this graph that roughly 75% of left-handed children were being forced to use their right hand anyways.
Many trans people, including me, will tell you that the world was not safe for trans people 30 years ago. Very few trans people were “out” at the time. I didn’t even know the word until college (early 2000’s). Pop culture mocked trans people31. Like I said above, huge changes to the medical situation around trans people happened in the early 2010’s. Today, I know so many trans people with the same story as me — I could not safely understand my gender until very recently. Growing up now, I would have known, and could have pursued medical transition as a teen and young adult. But I didn’t grow up now, so I didn’t transition until I was 40.
In any case, yes, the numbers in the 2010’s grew rapidly. But they have also leveled off. But anyone trying to say that the increased numbers are due to (completely unevidenced) social contagion while refusing to engage with the fact that prior years were suppresed is showing tremendous bias. The latter is evidenced by every trans person with a story like mine, as well as simply the known fact of transphobia32 through the years33). But perhaps most directly: it’s evidenced by the fact that “social contagion” is literally used as an argument to deny trans people the ability to live as themselves.
The argument of social contagion attempts to say that transness is generated via social influence (with no solid evidence), when we have decades of history, including the use of the “social contagion” argument itself, of tremendous societal pressure preventing trans people from transitioning.
Regardless, despite this increase, we still see very high satisfaction among those who transition. Unless we see a substantial decrease in that satisfaction, there is every reason to believe that what we are seeing is simply closer to the true number of trans people, who are now visible with the stigma reduced.
Finally, Dr. Sprinkle mentions similar growth trends in other countries, which I have no disagreement with.
Concern
After that, he says this, with no citation:
A growing number of medical practitioners, feminists, parents, detransitioners, and even some older trans* people are deeply concerned about the sudden rise in young people questioning their gender.
I don’t want to spend too much time on this because there is no source. But I will say this:
Every major medical organization in the US supports gender-affirming care. No European country that allowed gender-affirming care has now banned it, not even the UK.
Yes, there exist trans-exclusionary radical feminists (“TERF’s”), who are, as the name implies, anti-trans. But women in general are more supportive of trans people, not less, despite all of the hand-wringing about “women’s spaces” and “women’s sports,” which are issues which affect women directly.34
It’s impossible to evaluate his claim about parents.
We already discussed detransitioners who regret their transition - a “growing number” is likely true, but there is no evidence of a percentage that is either growing or concerning.
“Even some older trans* people” - as with any group, you can find someone from a marginalized group who is willing to agree with the points of the majority. These trans people do not speak for the whole, just like I don’t. But the vast majority of trans people support youth having access to appropriate gender-affirming care - this is not a large debate within the community.
Then Dr. Sprinkle goes on to describe his own experience as an evangelical Christian who speaks against gender transition.
Through my own organization, the Center for Faith, Sexuality & Gender, I’ve seen a dramatic increase in emails and phone calls from parents whose child comes out as trans*, seemingly out of the blue, with no prior evidence of gender dysphoria. Many of these stories that I’ve listened to fit the description of ROGD.
First, Dr. Sprinkle cannot diagnose someone as having ROGD because:
ROGD doesn’t exist as a diagnosis
Dr. Sprinkle is not someone with a credential that would allow him to diagnose anything
Second - I have no doubt that a man who is known for speaking against LGBTQ+ people in the church gets calls and emails from anti-LGBTQ+ parents.
And third, because of that, it’s not surprising at all that those parents would be caught off guard by their child coming out. Coming out, almost by nature, is something that happens “suddenly”. My parents never knew of my struggle with gender dysphoria until the moment I told them I was transgender. To them, I would fit the description above, “parents whose child comes out as trans*, seemingly out of the blue, with no prior evidence of gender dysphoria.” What this completely omits is any discussion with the child as to what prior evidence they have for gender dysphoria. I had decades of it, despite my parents not knowing. I hid it all that time, terrified that anyone would find out, because of what they would think of me. When I did start to come out, I told the safest people first, and then gradually more. I was already on Hormone Replacement Therapy (HRT) by the time I came out to many people.
And this is the thing - almost definitionally, a parent does not know that a child is trans until the child says they are trans. At which point the child has likely been thinking about it for a while, but the parent is hearing it suddenly. If the parent won’t listen, and won’t hear the child say “this is how it has been for me”, then the parent may look for a theory like ROGD to say, “something made my child trans.” And if the ROGD narrative has been pushed through the media, churches, and conservative books and online spaces, along with anti-trans sentiment, then the parents find exactly the theory they need to dismiss their child, and they adopt it.
But let’s further talk about selection bias - Dr. Sprinkle is a conservative evangelical author, known for his “let’s be nice, but still not affirming” position towards LGBTQIA+ people. What type of parents are going to email him for advice? Those who fundamentally support their trans child? Or those who do not? And when he (or someone else) offers them the narrative of ROGD, when they desperately want to believe that their child isn’t “actually” trans, these parents are likely to accept it, despite what their child is saying.
I’m not the first to come to this conclusion: gender dysphoria is not a social contagion. But the belief that it is one very well may be. It’s an idea that spreads without evidence, contrary to actual evidence.
To be continued…
I know we haven’t gotten to it yet, but the next section gets into Dr. Sprinkle’s actual discussion of the study written by Lisa Littman on the concept of ROGD. We’ll dig into both the study and his writing about it. It’ll probably take a couple posts to get through it, but one of them is almost finished, so expect it in the coming days.
Before you go, please don’t forget to subscribe to make sure you get the next part, and to let me know you appreciate my work - it really does help, and it’s free! Also, leave comments, questions, etc below - I always read them, I try to respond, and they help me know what you’d like to hear more about.
Source: “All the evidence against transgender social contagion”, Julia Serano, February 21, 2023.
We’re starting on page 161 here
Source: US Transgender Survey, page 17.
Source: Associated Press: “How common is transgender treatment regret, detransitioning?”
Yes, you are welcome to hold me to this standard when I’m trying to share information. Of course, an opinion can include emotional language, and Dr. Sprinkle is welcome to do that. But for something like this, “numbers have risen by [some] percent over [some] years” is much more appropriate than introducing the topic with a word like “exploded.”
The footnote (I’ve added the link): “See Lisa Marchiano, “Outbreak: On Transgender Teens and Psychic Epidemics,” Psychological Perspectives 60, no. 3 (2017): 345–66.
Sprinkle, Preston M.. Embodied: Transgender Identities, the Church, and What the Bible Has to Say (p. 271). (Function). Kindle Edition.
Whose credentials include: LCSW (Source: Interview with Feminist Current); Certified Jungian Analyst (Source: Marchiano’s Personal Website); Presently working on a Doctorate in Psychoanalsis and Psychotherapy (Source: LinkedIn)
The phrase was “rapid onset of gender dysphoria”, and it was used in July, 2016, in recruitment posts for the survey that ultimately was used in Dr. Littman’s now-corrected study, “Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports”.
This is according to Marchiano herself in an October 2016 podcast(here, transcript here), in which she says she became aware of transition through the news and through clients of hers who had trans family members. She explicitly states that she has not worked with detransitioners in a professional capacity. When she wrote the “Outbreak” article in October 2017, there is no new experience mentioned.
Dr. Littman herself is not in a mental health field at all.
Source: Reuters: “Putting numbers on the rise in children seeking gender care”. This is the most comprehensive report recently, and it has data from 2017 to 2021. Notably the number of youth (age 6-17) receiving a new gender dysphoria diagnosis increased from 15,172 in 2017 to 42,167 in 2021, with a particularly large jump in the first year of the Biden administration (24,847 new diagnosis had been reported in 2020, the final year of the first Trump administration). It is worth remembering that these are new diagnosis, so each year should be thought of as the increase from the previous year, not the new total. Since this report doesn’t have numbers that go back farther, it is difficult to say what the total was, though even just among this set, that 42,167 represents roughly 34% of the 121,882 minors diagnosed withg ender dysphoria in that five years. Put another way, it increased the total by roughly 52% from the previous year, the largeset increase in any year. My hypothesis (admittedly untested) is that this would have been primarily due to the Biden administration being far more trans-friendly than the Trump administration, and so youth and their families may have been more comfortable seeking diagnoses once Biden was in office.
Surgeries are even more rare - at less than 300 total per year, nearly all of which are double mastectomies. There were fewer than 60 genital surgeries done on minors in the three year period, making these vanishingly rare, at a rate less than two a month, across the entire country.
Source: NBC, reporting on a study by the CDC: “About 3% of U.S. high schoolers identify as transgender, national survey finds”
A previous version of this essay included a fragment of a note about the linked CDC study, which was just an editing error, as far as I can tell. I’ve removed it.
The title of Abigail Shrier’s anti-trans book, which I will not link.
The Cass Review has been critiqued or debunked by, among others: Yale, the medical group representing Germany, Switzerland, and Austria, the British Medical Association, and another paper here). Julia Serano has an excellent article about it here, which in turn pointed me to Dr. Ruth Pearce’s “Round-up” page with dozens if not hundreds of links to organizational and expert reviews of it. Abigail Thorn (YouTube channel: PhilosophyTube) has called it a document which is meant to be cited, not actually read, a concept she and Ian Danskin explore in their outstanding joint YouTube Video: “The Alt-Right Playbook: Double Wrong”. The podcast Maintenance Phase also spent three episodes on the concepts of ROGD and the Cass Review (starts here).
Source: Julia Serano “Reframing ‘Transgender Desistance’ Debates,” (2018) which in turn references her article from 2016, “Detransition, Desistance, and Disinformation: A Guide for Understanding Transgender Children Debates.”
Source: On Dr. Sprinkle’s “Theology in the Raw” podcast, he interviewed Dr. Paul Eddy. Dr. Eddy was commissioned by Dr. Sprinkle’s organization to write a paper on detransition. In the podcast, Dr. Eddy states ““And then now the statistic you're going to see increasingly among affirmative folks today is actually dropping 0.3 to 0.6 (percent). You're going to start seeing that more and more. And here's the reason why. A 2018 study by Weepjaz et al., it's another European group, found this stat that female to male, regret rate 0.3, male to female 0.6, so below 1%. And I'm starting to see that study statistics being replicated now.”
From Theology in the Raw: What Do We Actually Know about Transition Regret and Detransitioning? Dr. Paul Eddy, Jul 18, 2024
Billie Hoard and I actually have spent five YouTube videos so far talking about the that interview between Dr. Sprinkle and Dr. Eddy on detransition, going through their claims. More to come after publishing this article, including the next section, which will be on ROGD itself.
Source: “A systematic review of patient regret after surgery- A common phenomenon in many specialties but rare within gender-affirmation surgery” (Thornton, Sarah M. et al)
Source: Forbes, “Revealing Divorce Statistics In 2025”
Source: “Sex Assigned at Birth Ratio Among Transgender and Gender Diverse Adolescents in the United States” (Turban, Jack et al)
Source: Julia Serano, “Explaining Assigned Sex Ratio Shifts in Trans Children”
Source: Reuters: “Putting numbers on the rise in children seeking gender care”.
This footnote takes the reader to a defunct link about the GIDS service itself, and a “lengthy discussion” by GenderHQ, which does support the numbers that Dr. Sprinkle presents.
Davies, A., Bouman, W. P., Richards, C., Barrett, J., Ahmad, S., Baker, K., … Stradins, L. (2013). Patient satisfaction with gender identity clinic services in the United Kingdom. Sexual and Relationship Therapy, 28(4), 400–418. https://doi.org/10.1080/14681994.2013.834321
2,750 children in 2019-2020, vs. a population of roughly 4.5 million in the UK aged 12-17 in 2019 (from this spreadsheet, from this UK government website)
The UK Financial year ended on March 31st (as it always does), roughly two weeks after the first advisory on staying at home if you can was issued in the UK (March 16), and a week after the stay at home (March 31) was issued. If we assume that these two weeks dropped to zero (and given that these are medical services, which may have continued during lockdowns, that’s no guarantee), that would result in roughly a 4% reduction in annual numbers.
See Lindsay Ellis’ video essay, “Tracing the Roots of Pop Culture Transphobia”
Like the Nazi burning of the research records at the Institute of Sexology in Germany in 1933. (Source: Holocaust Memorial Day Trust)
Like the police raid that prompted the Stonewall Riot, as well as modern attempts to erase the history of the role of trans people at Stonewall. (Source: Caelan Conrad and Sarah from the Leftist Cooks; Source: Erin Reed)
Source: Pew Research, “Americans’ Complex Views on Gender Identity and Transgender Issues”