
The Sweetest Poisons: Part 10C
Dr. Lisa Littman and the (heavily corrected) study on "ROGD"

As we have before, let’s continue to remember this1:
…if trans people are imagined to be “contaminating” and capable of “infecting” or “converting” others (whether via “social contagion” or “grooming”), then that provides a convenient excuse for those who wish to “quarantine” us (e.g., by preventing us from participating in society, censoring our life experiences and perspectives, or perhaps even eliminating us all together).
Julia Serano - “All the Evidence Against Transgender Social Contagion”
Note on this post: This is part of a series, started by my friend Billie Hoard discussing Dr. Preston Sprinkle’s book Embodied. You can see the whole index for the series here. This is the third part of Chapter 10. Previously:
Part 10A: I discussed how the entire concept of Rapid-Onset Gender Dysphoria (ROGD) is junk science (technical term2), not to be taken seriously. I also discuss Dr. Sprinkle’s first example of a woman who detransitioned, and how he forces her story to fit his narrative more neatly.
Part 10B: I discuss Dr. Sprinkle’s invocation of three anti-trans talking points. Specifically, the fast growth in teens seeking gender-affirming care in the 2010’s, the shift towards more trans boys getting care than trans girls, and once again, detransitioners.
This post will cover the third part of Chapter 10, in which Sprinkle introduces Lisa Littman and begins discussing her study.
The Study
This entire post needs to be read through the lens that Gender-affirming Care is endorsed by every relevant major medical organization in the country as being the best treatment for gender dysphoria in youth and adults. It’s been studied for decades and shows phenomenal satisfaction rates for patients. It’s cautious, requiring multiple evaluations over months or years for a teenager to get puberty blockers or hormones. Surgeries are rarely performed on minors, and when they are, the rigor of those evaluations and the time to receive treatment increases. No one is pushing anyone into transition.
Meanwhile, the study that backs claims of ROGD is one that only produced a hypothesis, which has not been substantiated, and has significant evidence against it.
Despite that, many who are anti-trans use ROGD as a way to invalidate trans identities, at times positioning it as settled fact, outweighing all of the other research.
I made this meme to illustrate this posture:

The Author: Lisa Littman
Lisa Littman is the author of the original study on what she called “Rapid-Onset Gender Dysphoria.” Dr. Preston Sprinkle introduces her this way:
Lisa Littman of Brown University coined the term Rapid-Onset Gender Dysphoria “rapid-onset,” because most of these kids announce they are trans* in a way that seems quite sudden to their parents and counselors.
Littman’s credentials are conspicuous for their absence beyond “of Brown University.” She is not someone who had ever worked professionally with a child experiencing gender dysphoria. She is a medical doctor, yes, but she is an OB/GYN3. She has worked in “public health”, but her projects were, according to her, “mostly related to the health of pregnant women (immunizations, smoking cessation, oral health, premature births)”.4 Which is to say, she has no relevant experience when it comes to research on gender dysphoria, nor does she have a co-author who does. The lack of a co-author with relevant experience, in my opinion, is somewhat damning. It could imply that she cares so little about expertise that she didn’t look for one. Alternatively, it may indicate that all experts she approached either did not view her as worth partnering with or her study as something on which it would be worthwhile to collaborate.
Dr. Sprinkle’s wording, “because most of these kids…,” is completely unfounded — it’s not even a claim Littman herself made in her study. As we discussed in the previous entries, she coined the term during the development of the study, not as a conclusion. Therefore, it could not have been based on an empirical “most” yet, as no study that could have yielded such a characterization had been done. Moreover, the design of her study (as we will discuss) is incapable of saying what percent of trans teens experience her hypothesized “ROGD”, as it explicitly only accepted responses from parents who believed their children had experienced a rapid onset of gender dysphoria. If I did a study asking for people who got a sudden flat tire whether or not the tire experienced any damage, I would expect 100% of responses to tell me they experienced a sudden flat tire, which does not indicate that 100% of flats are sudden or that 100% of drivers experience flat tires at all. Finally, as Littman had not yet — and still has not — verified the existence of ROGD, let alone the rate at which it occurs, those cannot have been the reason she coined the term, as Dr. Sprinkle claims. Dr. Sprinkle’s claim here is entirely false.
There is one thing Dr. Sprinkle deserves credit for, which is that he includes the phrase “seems quite sudden to their parents” (emphasis mine). The omission of the fact that this study is about parent reports is a key weakness of much reporting on this study, and indeed the original study fails to consistently present things from this perspective. Sadly, Dr. Sprinkle will not maintain this phrasing, but it’s notable that he includes it up front.
We continue:
A few years ago, Littman published the first peer-reviewed study on ROGD…
And with that, before we go any further, we need to talk about the massive correction this paper went through.
The Correction
I’m going to rip the Band-Aid off right now. The study56 was released on August 16, 2018. Criticism of it mounted quickly enough that just eleven days after publication, on August 27th, a formal review was announced by PLOS One, the journal that published it7. In March 2019, a massive correction8 was published, and the editor-in-chief of PLOS One issued an apology to the “trans and gender variant community.” From what I found, this is the only apology ever issued by PLOS One9, a journal which publishes tens of thousands of papers per year10. The correction included a new Title, Abstract, Purpose, Methods, Results, Conclusion, and more.
Dr. Sprinkle never mentions the existence of this correction, either in his main text or in his footnotes. His footnote (later in this paragraph) uses the corrected title of the paper, so he was almost cetainly aware of it but chose not to provide this information to his readers. For him to have an entire chapter devoted to the concept of “ROGD” without even mentioning that the foundational study underwent a significant correction, is misleading to the point of dishonesty, unless he is unthinkably sloppy, biased, or both in his research.
Littman’s original conclusion11 says, “Rapid-onset gender dysphoria (ROGD) describes a phenomenon…,” implying that its existence has been confirmed. The corrected conclusion12 instead states, “Emerging hypotheses include the possibility of a potential new subcategory of gender dysphoria (referred to as rapid-onset gender dysphoria) that has not yet been clinically validated…“ Here, we see that the study simply gathered information that lead to the “generation of hypotheses” and that, “More research that includes data collection from AYAs, parents, clinicians and third party informants is needed…”
Littman writes this about the correction13:
As mentioned in the article, the study design of this research falls under descriptive research: as such, it did not assign an exposure, there were no comparison groups, and the study’s output was hypothesis-generating rather than hypothesis-testing [12]. Descriptive studies often represent a first inquiry into an area of research and the findings of descriptive studies are used to generate new hypotheses that can be tested in subsequent research [12–13]. Because of the known limitations of descriptive studies, claims about causal associations cannot be made [12], and there were none made in the article. The conclusions of the current study are that the findings raise certain hypotheses and that more research is needed.
Let me re-emphasize: “claims about causal associations cannot be made.” And then we again see the call that, “more research is needed.”
The “Formal Comment”14 published by PLOS One alongside the correction acknowledges that parent perspectives are interesting scientifically, but discusses their limitations at length, suggesting two alternative study designs that would have been better. It particularly takes exception with trying to establish a new diagnosis with no input from the youth involved:
Several studies have pointed out the importance of involving young people in studies of their health [2]. From a bioethical point of view, despite several dilemmas [3], this need is guided by the principle of the best interest of children and their right to be represented in the matters that affect them [4]. In this regard, with respect to medical procedures related to gender in childhood (in trans and intersex cases), the WHO among other agencies [5], already recognized the need to take children’s voices into account in order to avoid coercive treatments: "the best interests of the child should always be the primary concern, giving due weight to the views of children in accordance with their age and maturity, and taking into account their evolving capacity for decision-making" (p13).
Not only does it highlight scientific support for including youth perspectives, it cites both the United Nations and the World Health Organization regarding the rights of youth to have their perspectives included and the importance of doing so to prevent “coercive” treatments.
The “Formal Comment” is well worth reading in its entirety.
Importantly, despite the “generation of hypotheses” and the emphasis on a need for more research, Littman has performed a follow-up study. However, others have, which I’ll discuss later, but Julia Serano’s thorough essay All the Evidence Against Transgender Social Contagion15 covers the relevant research and I recommend reading it in its entirety.
Study Discussion
Dr. Preston Sprinkle begins his discussion of the study with this:
A few years ago, Littman published the first peer-reviewed study on ROGD, where she surveyed 256 parents who have kids (83 percent of whom are female) that seem to fit her description of ROGD.[12]16
First, despite Dr. Sprinkle’s later argument in his book to use the pronouns a trans person prefers, he misgenders the kids instead of using “assigned female at birth.”
Now, let’s look at how this study was performed.
In July of 2016, Lisa Littman posted an invitation to a survey on three online forums which are self-described in anti-trans terms: 4thwavenow, transgendertrend, and Youth Trans Critical Professionals. According to Littman’s correction, it was also shared (not by her) to a Facebook group, “Parents of Transgender Children”17, though that share is not publicly available, nor do we fully understand the composition of that group. While that may have added some responses from parents who were not anti-trans, the survey itself has a strong filter on who could take it, which I will discuss in a moment.
The link to the survey was also promoted by conservative writer David French in an article in National Review introducing his readers to the ideas of “rapid onset gender dysphoria” and “transgender contagion.”18 His article unbelievably pushes this idea as established fact while promoting the survey that informs the first ever study into whether or not it’s even a warranted hypothesis. From this, we can establish that some conservative voices were ready to run with the idea even without any scientific backing for it.
The survey invitation is quite interesting19, and I want to quote the opening to it:
We have heard from many parents describing that their child had a rapid onset of gender dysphoria in the context of increasing social media use and/or being part of a peer group in which one or multiple friends has developed gender dysphoria and come out as transgender during a similar time frame. Several parents have described situations where entire friend groups became gender dysphoric. This type of presentation is atypical and has not been studied to date. We feel that this phenomenon needs to be described and studied scientifically.
If your child has had sudden or rapid development of gender dysphoria beginning between the ages of 10 and 21, please consider completing the following online survey.
Furthermore, in the analysis of the data they received, they explicitly rejected responses that did not fit the ROGD narrative. According to the study itself:
Inclusion criteria were (1) completion of a survey with parental response that the child had a sudden or rapid onset of gender dysphoria; and (2) parental indication that the child’s gender dysphoria began during or after puberty. There was logic embedded in the survey that disqualified surveys that answered “no” (or skipped the question) about whether the child had a sudden or rapid onset of gender dysphoria and 23 surveys were disqualified prior to completion (20 “no” answers and 3 skipped answers). After cleaning the data for the 274 completed surveys, 8 surveys were excluded for not having a sudden or rapid onset of gender dysphoria and 10 surveys were excluded for not having gender dysphoria that began during or after puberty, which left 256 completed surveys for inclusion.
As you can hopefully see with this study design, Dr. Sprinkle’s “most of these kids” cannot be supported by this study, anymore than a study on the experiences of left-handed trans kids could establish that “most of these kids” are left-handed.
In a court, this would also be known as “leading the witness.” This invitation amounts to something like, “We want to show that ROGD is a thing. If you believe that ROGD is a thing, tell us that ROGD is a thing.” It’s not just selection bias of placing the invite on anti-trans sites, it explicitly asks for only parents who believe that their children experienced “a rapid onset of gender dysphoria.” It even tells them the hypothesized causes (social media and peer groups), prior to asking participants to characterize these things in their kids.
As for the methodology, this survey was an anonymous survey on SurveyMonkey. Literally anyone could respond to it, and no personally identifiable information was collected. No effort was made to ensure or confirm that the responses were coming from real parents or that they accurately described their children. I obviously cannot say with confidence that anyone was creating false or duplicate responses, but Littman cannot confidently state that no one did.
And this leads us to one of the biggest issues with the survey: only parents were even intended to be surveyed. The children, the ones who the survey is supposed to be about, were never spoken to. Dr. Sprinkle will discuss this issue in a bit, and I’ll save further discussion for when he does.
“Common factors”
Dr. Sprinkle then highlights some “common factors” that the parents reported.
Popularity and friendship
Some of these, like, “Many, if not all, of their friends at school were trans*, and their coming out often followed their friends’ coming out as trans*,” are impossible to verify from the parents’ perspective, especially given that the survey invite itself tells respondants this is one of the theorized factors.
One Dr. Sprinkle highlights is, “Many of them became more popular after they came out as trans*.[14]” Here, Dr. Sprinkle is paraphrasing in a way that changes the meaning substantially. The actual quote, which he only includes in footnote 14, is this (emphasis mine):
More than 60 percent of the kids Littman studied “experienced an increased popularity within their friend group when they announced a transgender identification”
I’ve heard this claim so many times - that kids are transitioning to be cool. But let’s look into the facts here.
Once again, no kids were studied. Parents were interviewed. The failure to frame things this way was one of the reasons the study underwent such a large correction. Here, Dr. Sprinkle just makes the same error again. But beyond that, Dr. Sprinkle omits the key phrase “within their friend group.” Even if we are taking the parents’ word as being accurate, they didn’t even claim that popularity at the school level reliably increased. Just within the child’s friend group. It’s also unclear how exactly the parent was evaluating this metric.
In fact, one of the “benefits” Littman says that parents described was that the child experienced, “improved protection from ongoing bullying.” That’s hardly an indication of a wide-spread increase in popularity, and in fact shows more of what trans people know is true: that we experience hostility at far greater rates than many other groups. According to the 2019 CDC Youth Risk Behavior Surveillance report20, which would have been available as Dr. Sprinkle was writing Embodied.
“29% of transgender youth have been threatened or injured with a weapon on school property, compared to 7% of cisgender youth…”
“43% of transgender youth have been bullied on school property, compared to 18% of cisgender youth”
“29% of transgender youth have attempted suicide, compared to 7% of cisgender youth”
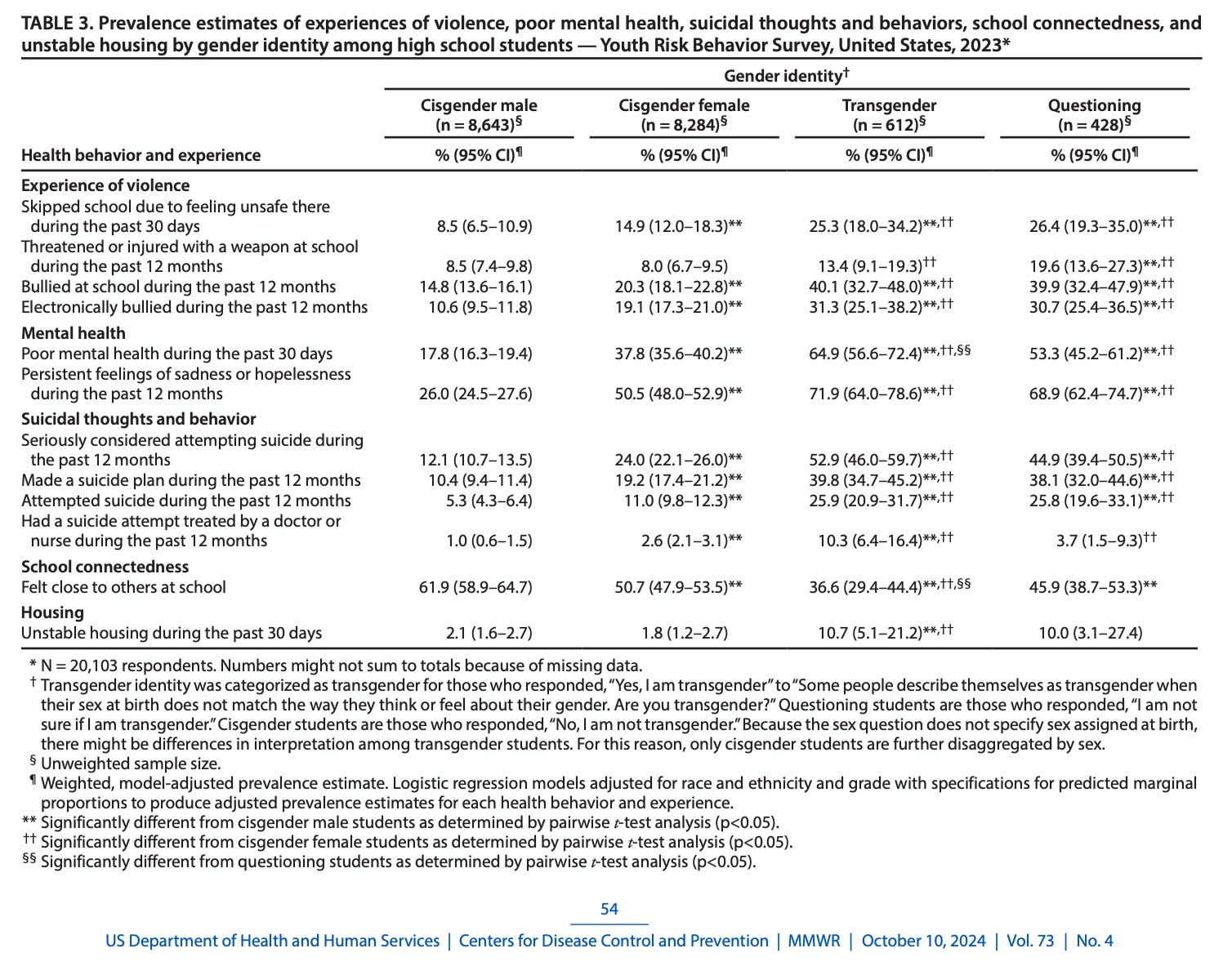
In 2023, the updated CDC report21 included more comprehensive data on youth who either identified as transgender or were not sure of their gender identity. The findings, I hope you’ll agree22, are beyond concerning. I’ve simplified the results table23 for ease of reading here:

These numbers are alarming and also include clear reasons for why mental health is so bad amongst those who are trans or questioning: high rates of bullying and lack of feeling safe, along with unstable housing and lack of social connection. Far from becoming more popular overall, trans and questioning kids are more likely than not to have a shortage of close connections at school.
Social Media
The next point Dr. Sprinkle lists is:
They engaged in heavy online and social media activity (more than normal) surrounding their coming out.
The study also doesn’t give any metrics or comparison to other children of the same age, so there’s not much to discuss here.
Mental Health
Dr. Sprinkle’s last common factor, which he spends some time discussing: “Many of them had other mental health concerns that weren’t being dealt with.”
That last point about co-occurring mental health concerns is significant. In fact, 63 percent of the kids referred to in Littman’s survey “had one or more diagnoses of a psychiatric disorder or neurodevelopmental disability preceding the onset of gender dysphoria.”
Once again, this statement is one the paper cannot (and does not) say24 - it can only say respondents reported the child had one or more of those diagnoses preceding the parents’ awareness of their child’s gender dysphoria. I’ll edit his language going forward.
He then lists multiple diagnoses, each of which I’d like to briefly comment on. Before I do, I want to bring up a data point that Dr. Sprinkle does not. Specifically, 195 (77%) of the 255 responses answered “No” to “Do you think your child is CORRECT in their belief that they are transgender?” Only six (2%) thought their child was correct25. That fits with the general tone of the three communities and again points to the selection bias. Let’s look at the supposed diagnoses:
“48% had experienced a traumatic or stressful event prior to the [respondents’ awareness of the child’s gender dysphoria].”
“Experienced a traumatic or stressful event” is not a diagnosis (This is Dr. Sprinkle’s error, not Littman’s), especially given the list of events in the survey, which includes the divorce of parents, a mental disorder in a sibling, or a break-up26. But more importantly, is Dr. Sprinkle really trying to argue that someone can’t know that they are transgender because they went through a breakup, or because their sibling has anxiety? Or on the flip side, is he trying to argue that parents divorcing could turn a child trans?
“45% were engaging in nonsuicidal self-injury prior to [respondents’ awareness of the child’s gender dysphoria].”
Again, that should read “prior to the parents’ awareness of the child’s gender dysphoria.” And this is largely consistent with surveys showing higher rates of self-harm and suicidality amongst those experiencing gender dysphoria, when not supported or permitted to transition. A 2023 systemic review of 21 other studies found that “[adolescents experiencing gender dysphoria] have more suicidal ideation, life-threatening behaviour, self-injurious thoughts or self-harm than their cisgender peers.”27 This is actually evidence that the child was experiencing gender dysphoria.
“15% had been diagnosed with ADHD”
Beginning with this one, Dr. Sprinkle’s numbers are wrong, because they are from a different table, for a different question. While still within a paragraph preceeded and followed by assertions that these numbers represent the children prior to coming out (Table 4 of Littman), Dr. Sprinkle is quoting numbers from Table 9, which include the time period after the child came out. I’ll correct the numbers as we go28.
In this case the number prior to coming out is 11.6%29. This is consistent with this from the CDC: “An estimated 7 million (11.4%) U.S. children aged 3–17 years have ever been diagnosed with ADHD, according to a national survey of parents using data from 2022.”30 As with other factors, it’s unclear how exactly ADHD would lead someone to incorrectly believe they are transgender — Dr. Sprinkle doesn’t explain, and Littman’s paper doesn’t discuss this result from the survey.
The last four are:
“12% had been diagnosed with OCD.” (Should be: 8.4%)
“12% were on the autism spectrum.” (Should be: 8.0%)
“7% had an eating disorder.” (Should be: 4.8%)
“7% were bipolar.” (Should be: 3.2%)
Like ADHD, no explanation is given for how these factors might influence someone to wrongly think they are transgender. And without that link, these are simply a form of ablism and infantilization of those with these conditions. It’s quite offensive to imply that someone with an eating disorder, for example, has a diminished capacity for either understanding their gender or for making decisions about transition. This is a whole other claim beyond the (unproven) hypothesis of ROGD, and neither Dr. Sprinkle nor Lisa Littman attempt to justify it.
Dr. Sprinkle follows that list with:
These mental health issues were present before the kids came out as trans*.
Here, Dr. Sprinkle finally correctly uses “before the kids came out as trans*” (italics mine). But he also labels the entire list as “mental health issues”, when neither autism nor having “experienced a … stressful event” are mental health issues. Particularly with regard to autism, this is highly irresponsible of Dr. Sprinkle, who should be more careful when speaking about a highly misunderstood group. Sadly his treatment of those with autism here appears to match his treatment of transgender people throughout this book.
Then Dr. Sprinkle says:
Of those who consulted a gender therapist or physician for the purpose of pursuing transition, only 28 percent of clinicians chose to “explore issues of mental health, previous trauma, or any alternative causes of gender dysphoria before proceeding”—even after parents informed the clinicians of previously diagnosed mental health issues. [17] One parent “tried to give our son’s trans doctor a medical history of our son,” but “she refused to accept it. She said the half hour diagnosis in her office with him was sufficient.”[18]31
I have to say quite a bit about this paragraph. First, 59% of the parents said their child never saw a physician or therapist, which could be an indication of unsupportive parents never even taking their child to be evaluated by professionals.
Second, the “28 percent” number is only 21% in the paper32, while 26% replied “Don’t Know” and 53% responded “No”. Littman’s paper clarifies that “before proceeding” means “before proceeding with the evaluation,” not transition itself, which a reader might infer from Dr. Sprinkle’s quotation33. Furthermore, this sentance shows either Littman’s bias or unfamiliarity with gender dysphoria. There are no known “alternative causes of gender dysphoria”, including mental health or previous trauma. She is, of course, welcome to study this and develop hypotheses, but it’s hardly nefarious of specialists to not inquire about potential alternative causes when there are no known alternative causes. Either Littman (and Dr. Sprinkle) are unaware of this or they are mounting a critique of professionals who are following known best practices. Remember, neither Littman nor Dr. Sprinkle have treated patients with gender dysphoria, or have a license that would allow them to do so.
Regarding the doctor who refused a medical history, this story doesn’t add up. I have never once seen a doctor without providing a medical history (including any doctor who has treated me for gender dysphoria). If this doctor went on to prescribe puberty blockers or hormones without at least some medical history, my understanding is that they would be guilty of medical malpractice. The family should sue and should win. But it’s also possible, as the paper says about many of the parents34, that the child was only being seen for evaluation of gender dysphoria, not for treatment options, in which case a medical history would be irrelevant. The later detail that it was regarding a “half-hour diagnosis” supports this. Again, that’d hardly be nefarious, as a medical history is irrelevant to the diagnosis of gender dysphoria, which we’ll take a loook at now.
Let’s talk about what the criteria for gender dysphoria are, so that we can understand why the above are irrelevant. The criteria are:35
A marked incongruence between one’s experienced/expressed gender and assigned gender, of at least six months’ duration, as manifested by at least two or more of the following:
- A marked incongruence between one’s experienced/expressed gender and primary and/or secondary sex characteristics (or in young adolescents, the anticipated secondary sex characteristics)
- A strong desire to be rid of one’s primary and/or secondary sex characteristics because of a marked incongruence with one’s experienced/expressed gender (or in young adolescents, a desire to prevent the development of the anticipated secondary sex characteristics)
- A strong desire for the primary and/or secondary sex characteristics of the other gender
- A strong desire to be of the other gender (or some alternative gender different from one’s assigned gender)
- A strong desire to be treated as the other gender (or some alternative gender different from one’s assigned gender)
- A strong conviction that one has the typical feelings and reactions of the other gender (or some alternative gender different from one’s assigned gender)
The condition is associated with clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Importantly, none of those symptoms are symptoms of any other psychological condition. Which is to say, a diagnosis of gender dysphoria requires no differentiation from other diagnoses. “A strong desire to be treated as the other gender…” is not a symptom of ADHD, OCD, or eating disorders. “A strong conviction that one has the typical feelings and reactions of the other gender” is not a sign that someone is on the autism spectrum.36
According to the World Professional Association for Transgender Health (WPATH), providers should, “Assess the capacity to consent for the specific physical treatment prior to the initiation of [medical treatments].”37 For this purpose, it would be necessary to account for any psychological conditions which impact an individual’s ability to consent to health care (of any kind). But again, things like ADHD, OCD, eating disorders, or having gone through a past stressful event are not things that would preclude consent even if they were discussed.
This entire section is just difficult to grapple with - the statistics are somewhat interesting, but in no way cast doubt on gender-affirming care. The anecdotes appear to be designed to undermine faith in the ability of professionals to provide appropriate care, but are anecdotal and missing enough context that they could not be used to build a substantive case against gender-affirming care. Finally, several of Dr. Sprinkle’s word choices here are ableist and infantilizing of those with various conditions.
Accused of transphobia
Let’s continue:
Parents were often called “transphobic” or “bigoted” by their kids if they encouraged their child to wait longer before transitioning, if they recommended a comprehensive health evaluation before transitioning, or if they simply expressed concerns about transitioning.[19] Littman said that the majority of the kids in her study thought “transition would solve their problems,” and many of them “became unwilling to work on their basic mental health issues before seeking treatment.[20]3839
Dr. Sprinkle is doing some serious cherry picking in that first sentence. Yes, those were all reasons listed for why the parents said they were called transphobic. But they aren’t the only reasons. 64% of responses said they had been called “bigoted” or “transphobic” by their child40. Of those, 80%41 of parents said one of the reasons was, “Disagreeing with the child about the child’s assessment of being transgender.” And… yes? If a child says they are trans, and the parent is not just uncertain about it, but actively saying the child is not transgender, it doesn’t surprise me if the child calls them transphobic. Again, these are parents who hang out in online forums called things like “Youth Trans Critical Professionals” and “transgender trend”.
Additionally, the average parent who said they were called transphobic/bigoted cited 5.2 reasons for being called this. Given that the child was likely not saying “I believe you are transphobic for each of the following five reasons”, we should interpret this more as the child had called the parent transphobic in an environment where the parent had done this collection of things (and potentially more).
Also note that
But to Sprinkle’s point, given that we know that 80% of those who were called transphobic were those who disagreed that their child was trans, what do we know about the factors Sprinkle named?
“encouraged their child to wait longer before transitioning”
This is not actually one of the options in the survey - the closest match is, “Recommending that their child take more time to figure out if their feelings of gender dysphoria persist or go away,” (italics mine). 70% of those who were called bigoted or transphobic cited this as a reason, but a minimum of 72%42 of these also said they disagreed with the child’s assessment of being trans. So yes - if a parent tells a child “you’re not trans, and you should wait and see if your feelings go away,” it’s hopefully understandable to you why the child might assess their parents as “transphobic”.
“recommended a comprehensive health evaluation before transitioning”
The original study reports this as “recommending a comprehensive evaluation before starting hormones and/or surgery.” The original survey specifies “mental health” evaluation. This is the rarest reason listed. Only about 33%43 of the parents who were called bigoted/transphobic cited this reason. A minimum of 40% of them disagreed with their child’s assesssment of being trans.
“simply expressed concerns about transitioning”
Sprinkle adds the word “simply” which, as I’ve shown, is almost certainly untrue. These parents were voicing multiple objections. And the actual response here is “Expressing concerns for their child’s future if the child were to take hormones and/or have surgery.” 63% of those who were called transphobic/bigoted chose this answer, and 69% of those denied their child’s trans identity.
Five other reasons are reported by Littman, but Dr. Sprinkle omits them:
“referring to their child by the pronouns that they used to use before the announcement” (misgendering): 59% of those called transphobic/bigoted
“Telling their child that they thought hormones/surgery would not help them” (inserting themselves into the role of psychologists/psychiatrists, endocrinologists, and surgeons): 58% of those called transphobic/bigoted
“Calling their child by the child’s birth name” (deadnaming): 52% of those called transphobic/bigoted.
“Recommending that their child work on other mental health issues first to determine if they are the cause of their dysphoria” (inserting themselves into the role of psychologists/psychiatrists, to investigate something that is not a known cause of dysphoria): 52% of those called transphobic/bigoted
“Recommending therapy for basic mental health issues (not related to gender)”: 48% of those called transphobic/bigoted. This is the one answer that I’d frankly recommend for anyone. In isolation, it would feel like an overreaction by the teen. However, given that a minimum of 40% (likely higher) of these also disagreed with their child’s assessment of being trans, and likely more cited other highly problematic reasons, we can’t take it in isolation.
Here’s the full set of responses:
 74 31% 48% 59% Recommending a comprehensive (mental health) evaluation before starting hormones and/or surgery 50 21% 33% 40% None of the above 87 36% N/A N/A")
To me, it seems that in a survey where only 2% of parents agreed with their child’s assessment, it’s a show of remarkable restraint by the kids that 36% of them had not called their parents transphobic or bigoted.
Perhaps interestingly, Littman asked about three additional factors, but does not include them in the final report, nor does she say why she excludes them:
Telling your child that you think hormones and/or surgery would be harmful to them
Refusing to drive your child to a gender therapist, gender clinic or physician for the purpose of transitioning
Refusing to pay for appointments, medications, surgery related to transition
One could speculate as to why these were not included in the final report, but I think it’s worth noting that these answers are some of the stronger forms of pushback Littman asked about. If many parents selected these answers, it would perhaps be even more understandable that the child saw their parents as transphobic or bigoted.
But regardless, yes: if someone refuses to call me my name or pronouns, and tells me that I’m not actually a woman, I feel comfortable using the label “transphobic” or “bigoted” for this (though I personally tend to use “anti-trans”)44. If you disagree, the burden is on you to give me a coherent definition of “transphobic” that does not include those behaviors.
Either way, Dr. Sprinkle is missing, ignoring, or hiding facts that don’t help his case, and seemingly trying to portray these parents as poor victims of overzealous teens. We’ve talked about DARVO45 before — the tactic wherein someone who harms another will Deny, Attack, and Reverse Victim and Offender. It’s what’s being implied here by Dr. Sprinkle, and possibly also by Littman and the respondents completing the survey. Here we have parents who are denying their children the ability to live as who they say they are, and in many cases denying them even the ability to explore their gender identity. It boggles my mind that I have to say this, but forcing someone to live as a gender other than what they know themselves to be is unbelievably harmful. But by centering the labels the child places on the parent, we see the DARVO in action — the kids are said to be doing harm by accusing their parents (likely accurately) of transphobia and bigotry. We’re meant to feel sorry for these poor parents, when in fact these parents are, whether they know it or not, inflicting damage on their kids that lead to mental health issues they may be unpacking with therapists for decades46.
As for the claim about children being unwilling to work on their mental health issues before seeking treatment, we alredy talked about this. Someone assigned male at birth saying, “I am a girl,” is a sign of exactly one psychological condition: gender dysphoria. And the gold standard treatment for gender dysphoria is gender-affirming care. On the other hand, gender dysphoria is known to cause mental health conditions such as depression and anxiety. This is why, “let’s just resolve your depression before we treat your gender dysphoria,” is as ridiculous as, “let’s just fix this flat tire before we take the nail out of it.” Is it possible there are additional contributors to the depression? Sure, and therapy is good for anyone with (or without) mental health conditions. But it’s not going to resolve the gender dysphoria, and no child should be expected to fix depression that arises due to gender dysphoria without being able to proceed with gender affirming care.
As for me, my work with therapists treated my depression, anxiety, and PTSD while we moved forward with gender-affirming care.
To be continued…
Well, this got long again, though we covered another … checks notes … three pages. Coming up, we’ll cover Dr. Sprinkle’s descriptions of the reactions to Littman’s study, and a brief passage where he discusses the sex ratio amongst trans youth. After that, we’ll move into a section about “Medicalizing the Youth”. Then, he’ll visit detransition again, but we already covered much of that. Finally, we’ll see his closing passage “A Christian Response.”
Before you go, please don’t forget to subscribe to make sure you get the next part, and to let me know you appreciate my work - it really does help, and it’s free! Also, leave comments, questions, etc below - I always read them and they help me know what you’d like to hear more about.
Source: “All the evidence against transgender social contagion”, Julia Serano, February 21, 2023.
Source: Quilette Interview with Lisa Littman
Ibid
The original, uncorrected paper is available as a supporting file at the end of the correction. You can find it here.
Source: “Statement by PLOS ONE staff” in comments on the original paper, which reads:
PLOS ONE is aware of the reader concerns raised on the study’s content and methodology. We take all concerns raised about publications in the journal very seriously, and are following up on these per our policy and COPE guidelines. As part of our follow up we will seek further expert assessment on the study’s methodology and analyses. We will provide a further update once we have completed our assessment and discussions.
Source: PLOS One - “Correcting the scientific record on gender incongruence – and an apology”
Source: PLOS One “EveryONE” Blog, search term “apology”
Source: Wikipedia, “PLOS One - Output and Turnaround”
In full: “Rapid-onset gender dysphoria (ROGD) describes a phenomenon where the development of gender dysphoria is observed to begin suddenly during or after puberty in an adolescent or young adult who would not have met criteria for gender dysphoria in childhood. ROGD appears to represent an entity that is distinct from the gender dysphoria observed in individuals who have previously been described as transgender. The worsening of mental well being and parent-child relationships and behaviors that isolate AYAs from their parents, families, non-transgender friends and mainstream sources of information are particularly concerning. More research is needed to better understand this phenomenon, its implications and scope.
In full: “This descriptive, exploratory study of parent reports provides valuable detailed information that allows for the generation of hypotheses about factors that may contribute to the onset and/or expression of gender dysphoria among AYAs. Emerging hypotheses include the possibility of a potential new subcategory of gender dysphoria (referred to as rapid-onset gender dysphoria) that has not yet been clinically validated and the possibility of social influences and maladaptive coping mechanisms. Parent-child conflict may also explain some of the findings. More research that includes data collection from AYAs, parents, clinicians and third party informants is needed to further explore the roles of social influence, maladaptive coping mechanisms, parental approaches, and family dynamics in the development and duration of gender dysphoria in adolescents and young adults.”
Source: PLOS One - “Formal comment on: Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria”
Julia Serano: All the Evidence Against Transgender Social Contagion
Original Footnote: “Lisa Littman, ‘Parent Reports of Adolescents and Young Adults Perceived to Show Signs of a Rapid Onset of Gender Dysphoria’ PLoS One 13, no. 8 (2018).”
Source: PLOS One - “Correction… Updated Information about recruitment”
Source: David French, in National Review - “The Tragic Transgender Contagion”
For example, the 4thwavenow invitation.
See the write-up by Human Rights Campaign here: New CDC Data Shows LGBTQ Youth are More Likely to be Bullied Than Straight Cisgender Youth
This entire report, which covers all manner of risk factors for youth in America, is only available from the CDC at this time due to a court order requiring the department of HHS to not remove it. The page hosting it currently has a note that the Trump administration “rejects” it due to it promoting “gender ideology.” I feel the need to underscore that this page talks about risks for all American youth, not just trans youth, and that regardless of what one thinks about transgender identities, it’s horrific that they simply want to delete data that would help prevent bullying, homelessness, mental health issues, and more.
Full table here:
I am sorry to keep making this point, but it’s critical to understanding just how unsubstantiated this part of Dr. Sprinkle’s book is.
The remainder said either “Don’t Know” (38 responses, 15%) or “Other” (16 responses, 6%)
Marconi, E., Monti, L., Marfoli, A. et al. A systematic review on gender dysphoria in adolescents and young adults: focus on suicidal and self-harming ideation and behaviours. Child Adolesc Psychiatry Ment Health 17, 110 (2023). https://doi.org/10.1186/s13034-023-00654-3
I don’t accuse Dr. Sprinkle here of malice. The two tables look very similar and it’s easy to get them mixed up if one is not very familiar with the report. This more strikes me as carelessness than an actual attempt to include incorrect information.
Table 4
The numbers in square brackets are footnotes in Embodied, which cite Littman’s paper, pages 24 and 26, respectively.
This change is more easily explained and is somewhat understandable. It appears that, unlike the paper, Dr. Sprinkle removed “Don’t Know” responses and recalculated the percentage only including those who responded “Yes”, or “No” to the question.
Many of the respondents clarified that their child had seen a clinician regarding their gender dysphoria for evaluation only.
Section: “Clinical Encounters”: “Many of the respondents clarified that their child had seen a clinician regarding their gender dysphoria for evaluation only.”
Source is the DSM-5, via Psychiatry.org.
I first saw this through a Twitter thread by Zinnia Jones about the “hexagon” - which was a data visualiztion that showed different overlaps of different criteria, but that gender dysphoria’s six criteria were not part of the diagnosis of anything else.
WPATH Standards of Care, version 8, page 30; requirement 5.3f. See also, requirement 5.
The footnotes correspond to Littman’s paper, pages 21 and 33 respectively.
For what it’s worth, citation 19 referincing page 21 of Littman’s paper indicates that Dr. Sprinkle was working off of the original version of the paper (the same data is on page 24 of the corrected paper), despite the correction having been issued nearly two years prior to his book being published.
Math: Table 10 shows that 240 parents answered the question about being called transphobic or bigoted, and 87 said they had not been. That leaves 153 who were, or 64%.
Math: 123 of those 153, or just over 80%.
Math: Only 30 who were called bigoted/transphobic did not outright disagree. So while 107 of the 153 parents who were called bigoted/transphobic cited “recommending that their child take more time to figture out if their feelings of gender dysphoria persist or go away”, we know that at most 30 of them (and as few as none of them) had not also told their child that they disagreed with the child’s assessment. This means at least 77 of the 107 had also disagreed with the child’s assessment.
Math: 50 out of 153, or 33%.
A lot of anti-trans (or anti-gay) people will push back against called “transphobic” or “bigoted.” I know, because I once absolutely lost my cool when a bisexual man called me a bigot. I expected my minimal tolerance to somehow make up for the fact that I publicly stated that I was against same-sex marriage and thought that gay relationships were sinful. I’d say, “but I have a gay friend!” Or, “But I’m against discrimination targeting gay people!” (even though I had witnessed it first hand and did nothing to stop it). People might say “but phobia means fear and I’m not afraid of trans people.” Firstly, are they sure they’re not afraid of us? A huge amount of rhetoric around trans people involves supposed threats we pose to society in general and women and kids in particular. “Phobia” can also mean something like “repelled by” (think about hydrophobic materials, also known as water-repellant). However, it’s more important to know: this is a symantic game and nothing else. I personally use the word “anti-trans” in an effort to avoid getting sucked into symantics, but it’s important to recognize that people who play games with “transphobia” or ask “but really is bigotry” are typically just moving the conversation away from whatever anti-trans thing they did.
But that’s the thing. Too often, the one doing anti-trans or anti-gay stuff will define bigotry as “someone more anti-trans/anti-gay than me.” They somehow want to hold these views without anyone labeling them as having those views.
Dr. Sprinkle is, whether he wants to admit it or not, anti-trans. He is against us living as ourselves. He spreads incorrect information and narratives to persuade others to agree with him. If the word “transphobic” has any meaning, surely it includes, “people who think that no one (or vanishingly few exceptions) should be transgender.” Surely it includes people who refuse to talk to transgender Christians who say he is hurting them.
And if the word bigoted has any meaning at all, surely it includes people who hold these views as well. He may not like the word. He may think that his bigotry is justified and correct. But the word has a meaning and he fits it.
As many trans people, including me, will attest.